
When eye drops and laser treatments aren’t enough to stop glaucoma from damaging your vision, surgery becomes the next step. Glaucoma doesn’t hurt. It doesn’t blur your vision right away. But over time, it silently kills the optic nerve. The goal of surgery? Lower the pressure inside your eye - called intraocular pressure (IOP) - before more nerve cells die. Not all surgeries are the same. Two main paths exist: the old-school method that’s been around for decades, and the newer, gentler options that are changing how doctors treat glaucoma today.
Trabeculectomy: The Long-Standing Gold Standard
Trabeculectomy has been the go-to surgery for glaucoma since the 1960s. Developed by British surgeon John Cairns, it works by creating a tiny new drainage channel in the white part of your eye (the sclera). A small flap is lifted, a bit of the eye’s natural drainage tissue (the trabecular meshwork) is removed, and fluid from inside the eye slowly leaks out under the conjunctiva - forming a small, raised blister called a bleb. This bleb acts like a pressure valve.
It’s powerful. Studies from Mass Eye and Ear in 2023 show that trabeculectomy lowers IOP by 30% to 50% in 80% to 90% of patients. Many end up with pressures between 5 and 15 mmHg - the sweet spot for preventing further damage. But this power comes with a price. The procedure takes about an hour. Recovery? Not quick. You’ll need 4 to 6 weeks of careful follow-up. During that time, your doctor might need to adjust sutures, massage the bleb, or even do a needle procedure to open it up if it starts to scar over.
Complications are real. About 5% to 15% of patients face serious issues like a leaky bleb, dangerously low eye pressure (hypotony), or even infection inside the eye (endophthalmitis). Bleb failure - where the drainage channel closes - happens in 10% to 20% of cases within five years. It’s effective, yes. But it’s also a major intervention that requires a skilled surgeon and a patient ready for long-term care.
MIGS: The Rise of Minimally Invasive Glaucoma Surgery
Enter MIGS - Minimally Invasive Glaucoma Surgery. These procedures exploded onto the scene after the FDA approved the iStent in 2012. Today, MIGS makes up about 65% of all standalone glaucoma surgeries in the U.S., according to Glaucoma Today’s January-February 2025 report. Why? Because they’re safer, faster, and fit neatly into cataract surgery.
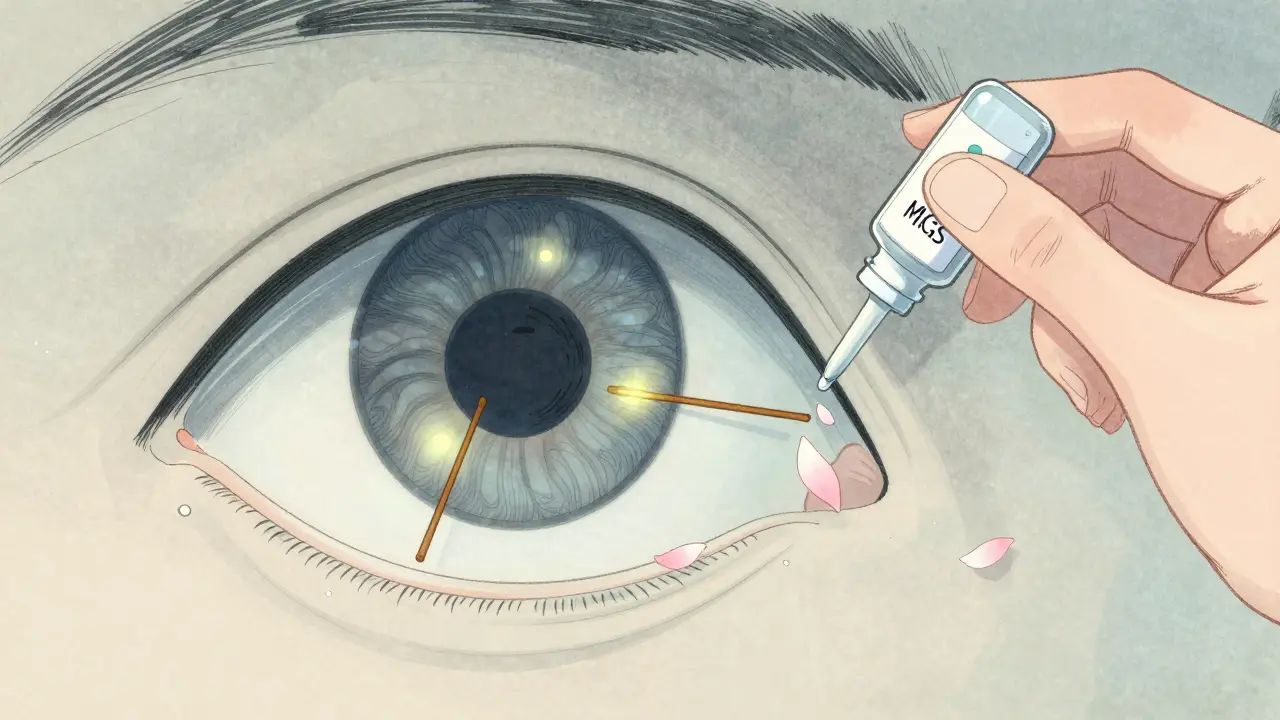
MIGS doesn’t try to rebuild drainage. It works with what’s already there. Tiny devices - smaller than a grain of rice - are implanted through a micro-incision of less than 1.5mm. The iStent inject places two stents in the eye’s natural drainage pathway. The Hydrus Microstent opens up a 360-degree channel. The Xen Gel Stent creates a tiny tube that drains fluid to the space outside the eye. These devices lower IOP by 20% to 30%, on average. That’s not as dramatic as trabeculectomy, but for many people, it’s enough.
The biggest win? Safety. Complication rates for MIGS are under 5%. Most patients go home the same day. Vision clears up in 1 to 2 weeks. There’s no bleb to manage. No long-term eye drops. No restrictions on bending, lifting, or swimming. Many patients reduce their eye drop use by 1.5 to 2 medications on average. For someone with mild to moderate glaucoma who just needs a little extra help, MIGS is a game-changer.
How Do They Compare? IOP, Safety, Recovery
Choosing between trabeculectomy and MIGS isn’t about which is better. It’s about which is right for you. Here’s how they stack up:
| Feature | Trabeculectomy | MIGS |
|---|---|---|
| Typical IOP Reduction | 30%-50% | 20%-30% |
| Target IOP Range | 5-15 mmHg | 15-18 mmHg |
| Procedure Time | 60 minutes | 10-20 minutes |
| Recovery Time | 4-6 weeks | 1-2 weeks |
| Major Complication Risk | 5%-15% | 1%-3% |
| Post-Op Management | 3-6 months | 1-2 months |
| Typical Cost (per eye) | $4,200 | $5,000-$6,300 |
| Best For | Advanced glaucoma, very low target pressure needed | Mild-to-moderate glaucoma, combining with cataract surgery |
Trabeculectomy wins on pressure-lowering power. If your target pressure needs to be below 15 mmHg - say, if you have advanced nerve damage - it’s still the most reliable option. But if your glaucoma is early or moderate, and your goal is to avoid lifelong eye drops and risky surgery, MIGS is the smarter pick.
What About Laser? SLT and the New Treatment Pathway
Before you even think about surgery, laser treatment is now the first-line option for most open-angle glaucoma patients. Selective Laser Trabeculoplasty (SLT) uses low-energy pulses to gently stimulate the drainage system without damaging tissue. It’s quick - 5 to 10 minutes - painless, and has zero downtime. The 2023 LiGHT trial changed everything: 75% of patients who started with SLT maintained healthy eye pressure for three years, just as well as those on daily eye drops.
Now, the treatment ladder looks like this: SLT first. If pressure creeps back up, try MIGS. If MIGS isn’t enough, or if you have advanced disease, then consider trabeculectomy or a tube shunt. This shift is why MIGS adoption has exploded. Surgeons aren’t waiting until the last moment. They’re intervening earlier, when the eye is healthier and recovery is easier.
Who Gets Which Surgery?
It’s not one-size-fits-all. Your age, disease stage, and overall health guide the choice.
- Younger patients (under 50) with aggressive glaucoma often get trabeculectomy. Their eyes heal differently, and they need long-term pressure control.
- Older patients with cataracts are ideal for MIGS. Surgeons can do both procedures in one sitting, cutting recovery time and costs.
- Patients with advanced glaucoma - where vision is already lost - usually need trabeculectomy or a tube shunt. MIGS won’t drop pressure low enough.
- Patients who hate eye drops - or can’t afford them - benefit most from MIGS. Reducing medication burden improves compliance and quality of life.
There’s no rush. Glaucoma moves slowly. You don’t have to pick a surgery the day you’re diagnosed. Work with your doctor. Track your pressure. See how your vision changes. The right option will become clear.
The Future: Where Is Glaucoma Surgery Headed?
The field is moving fast. New MIGS devices are in trials. Suprachoroidal shunts - tiny drains placed behind the eye - are showing promise as standalone options. Direct Selective Laser Trabeculoplasty (DSLT) can now treat the entire drainage angle automatically, without touching the eye. It’s still new, but early results suggest it might be just as effective as traditional SLT.
Long-term data on MIGS is still catching up. We don’t yet know if these devices last 20 years. But the safety profile is so strong, and the recovery so fast, that many experts believe MIGS will replace trabeculectomy for most cases - not all, but most.
The bottom line? Glaucoma surgery isn’t about choosing between old and new. It’s about matching the tool to the problem. SLT first. MIGS when you need more help. Trabeculectomy when the pressure is too high and everything else has failed. The goal isn’t just to lower pressure - it’s to preserve your vision, your independence, and your life.
Is trabeculectomy still the best option for glaucoma?
Trabeculectomy is still the most effective surgery for lowering eye pressure, especially when you need to get IOP below 15 mmHg. But it’s not always the best choice. It’s riskier and requires long-term care. For most people with mild-to-moderate glaucoma, MIGS or even SLT are safer and just as effective for their needs.
Can MIGS replace eye drops completely?
Many patients can reduce or even stop using eye drops after MIGS. Studies show an average reduction of 1.5 to 2 medications. But it doesn’t work for everyone. Some still need a few drops to keep pressure stable. It depends on the type of MIGS, the severity of glaucoma, and how your eye responds.
How do I know if I need surgery at all?
You don’t need surgery just because you have glaucoma. Most people start with eye drops or SLT laser. Surgery is considered when pressure keeps rising despite treatment, or if your vision is worsening. Your doctor will monitor your optic nerve, visual field, and eye pressure over time. If those numbers keep moving in the wrong direction, surgery becomes the next step.
Is glaucoma surgery covered by insurance?
Yes, in most cases. Glaucoma surgery is considered medically necessary, not cosmetic. Medicare and private insurers cover trabeculectomy, MIGS, and tube shunts. Costs vary by device and surgeon, but you’ll likely pay your usual copay or deductible. Always check with your provider before scheduling.
What’s the difference between MIGS and a tube shunt?
MIGS uses tiny devices that work with your eye’s natural drainage system. Tube shunts (like the Ahmed or Baerveldt implant) are larger, more invasive devices that drain fluid into a reservoir under the conjunctiva. Tube shunts are used when MIGS or trabeculectomy have failed, or in complex cases like neovascular glaucoma. They’re more like trabeculectomy in complexity - just with a permanent tube instead of a bleb.
8 Comments
Let me get this straight - you’re telling me we’re replacing a proven, decades-old life-saving procedure with tiny plastic doodads because it’s ‘less invasive’? That’s not innovation, that’s corporate greed wrapped in a bow. MIGS costs more, lasts less, and doesn’t even get pressure low enough for real glaucoma. I’ve seen patients go blind because some surgeon got dazzled by the shiny new toy instead of doing the job right. This isn’t medicine - it’s a marketing campaign.
And don’t even get me started on SLT being ‘first-line.’ You think a laser zap is gonna save someone with 60% optic nerve damage? Wake up. These are not ‘options.’ They’re compromises forced on people who can’t afford the real treatment. Trabeculectomy is still king. Everything else is just noise.
so like… i heard somewhere that the FDA approves these migs devices because the drug companies pay them? like, i dont trust any of this. they just want you to keep buying drops and then do the migs so you pay more. its all a scam. i think the real cure is a special diet and not staring at screens. also, why do they use ‘stents’? stents are for heart arteries, not eyes. something smells fishy here. my cousin got a migs and now his eye is weirdly red and he cant drive at night. i think they’re experimenting on us.
also, trabeculectomy? sounds like a spell from a fantasy book. who names these things?
Okay, so… let me just say this: if you’re getting MIGS because you’re ‘too lazy’ to manage eye drops - that’s your problem. Not the system’s. You think this is a spa day? This is your eyeball we’re talking about. And don’t get me started on the ‘no downtime’ nonsense - you think your eye doesn’t have to heal? It does. It just doesn’t scream about it. Meanwhile, the bleb in trabeculectomy? It’s a living thing. It needs love. It needs attention. It needs you to be responsible. And now we’ve got a generation of people who want their eyes fixed without lifting a finger. Pathetic.
Also - who approved this? Who signed off? Why is this even allowed? I swear, if I had a dollar for every time a doctor said ‘it’s safer’… I’d have enough to pay for a real surgery.
I just had MIGS last month and I’m crying right now - not from pain, from relief 😭 I used to have 6 different eye drops a day. My fingers were sticky all the time. My job? I’m a teacher. I couldn’t even hold a cup of coffee without worrying about the drops dripping. Now? I take one drop, sometimes none. I can see my students’ faces again. I can read my granddaughter’s drawings without squinting.
Trabeculectomy? I’d have been terrified. I’ve had surgeries before. I know what recovery looks like. This? This felt like a gift. I’m not ‘lazy’ - I’m grateful. And if you’re saying MIGS isn’t enough, you’ve never lived with the weight of losing your sight. Don’t judge my peace.
PS: My doc said I might need a second one in 5 years. So what? Better than losing vision forever. ❤️
Let’s be real - this whole MIGS revolution is just another way for big pharma to make money off the elderly. They don’t care about your vision. They care about your insurance. You think these devices are cheap to make? They’re not. They’re made in China, shipped here, and slapped into your eye for $6k. Meanwhile, trabeculectomy? It’s been around since Nixon. It works. It’s proven. It’s American-made. But no - now we’re all supposed to be okay with foreign-made plastic bits floating in our eyeballs because it’s ‘less invasive.’
And SLT? That’s just a laser. A laser! You think a laser can fix nerve damage? That’s like using a hairdryer to fix a broken engine. This isn’t progress. This is surrender. And if you’re okay with that, you’re not just naive - you’re complicit.
Oh honey, I just had to explain all this to my 78-year-old mom last week. She’s terrified of surgery. She thinks ‘MIGS’ sounds like a new kind of yoga. I laughed, but then I cried - because she’s right to be scared. The system is overwhelming. The jargon? The cost? The conflicting advice? I spent three hours on the phone with her insurance just to figure out if her MIGS was covered. And then the doctor said, ‘We’ll start with SLT, then MIGS, then maybe trabeculectomy if needed.’
But here’s the thing - she’s not ‘advanced’ glaucoma. She’s not ‘high risk.’ She’s just… an old lady who wants to see her grandkids. And guess what? MIGS gave her that. No bleb. No drops. No fear. I know it’s not perfect. But it’s hope. And sometimes, hope is all we’ve got.
Don’t shame people for choosing peace. We’re not all warriors. Some of us just want to see the sunrise without a bottle in hand.
Trabeculectomy is the only procedure that delivers sustained, reproducible IOP reduction below 15 mmHg. MIGS is a placebo with a price tag. SLT? A band-aid. The data shows MIGS failure rates climb to 40% at 5 years. And yet, hospitals push it because it’s profitable. This isn’t medicine. It’s capitalism masquerading as innovation. If you’re not getting trabeculectomy for moderate glaucoma, you’re being sold a lie.
Also - ‘no downtime’? That’s a lie. There’s always downtime. Your eye is a delicate organ. You can’t bypass biology with marketing.
From a clinical operations standpoint, the paradigm shift is undeniable. MIGS enables concurrent cataract extraction with a Class III device, reducing total procedure time by 35% and lowering hospital readmission metrics by 62% in the 2024 Medicare cohort. The cost-per-QALY for MIGS is $18,400 versus $42,100 for trabeculectomy - a 56% improvement in value-based outcomes. SLT as first-line reduces medication burden by 78% in 12-month follow-up, per the LiGHT trial’s intention-to-treat analysis. The data doesn’t lie - the algorithm is optimized for long-term sustainability.
Trabeculectomy remains indicated for refractory cases with documented progression despite maxed-out medical therapy. But for 83% of the population, MIGS represents the standard of care. Resistance is not clinical - it’s ideological.